Asthma Health Disparities in the United States
TRENDING NOW
● Puerto Rican Americans experience the highest asthma rates in the United States
● Climate change is worsening asthma disparities
● Breakthrough asthma treatments are not reaching those most at risk
Asthma is one of America’s most common chronic diseases, affecting more than 28 million children and adults and sending hundreds of thousands to emergency departments every year. It drives missed school, lost workdays, preventable hospitalizations, and in the most severe cases, death.
Asthma can often be managed successfully, yet the medications, care, and environmental conditions that make that possible are not shared equally across communities. The heaviest burden falls on people living in communities with more air pollution, substandard housing, and limited access to primary and specialty care — making asthma not just a medical condition, but a reflection of unequal living conditions and unequal access to safe air.
An average of nine people die from asthma every day in the United States. Almost all of those deaths are preventable and they’re not random. These are the facts that should organize everything else.
Part 1: Who Bears the Greatest Burden of Asthma
An average of nine people die from asthma every day in the United States. Almost all of those deaths are preventable and they’re not random. These are the facts that should organize everything else.
No group carries a heavier burden than Black Americans. They’re about twice as likely to die from asthma as white Americans and nearly six times more likely to visit the ER. Black children are nearly four times as likely to die as the national average, with ER visit rates of 89 per 10,000 versus 14 for white children. This gap is not narrowing.
American Indian and Alaska Native adults also have a high prevalence of asthma, compounded by geographic isolation, limited specialty care, and disproportionate exposure to the environmental conditions that trigger attacks.
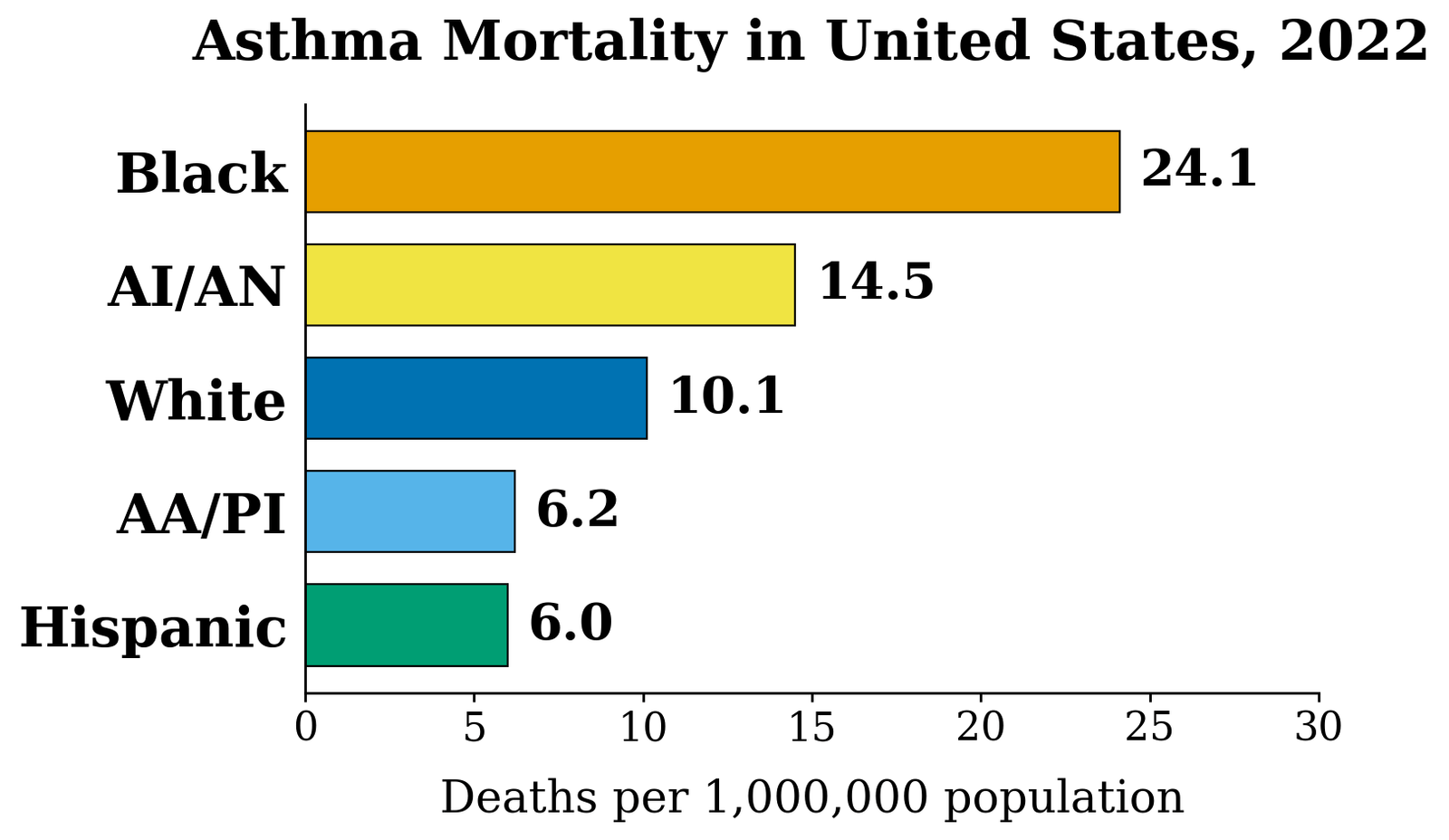
AI/AN=American Indian/Alaska Native; AA/PI=Asian American/Pacific Islander. Source: CDC, Most Recent Asthma Data, mortality table, 2022
Why is their rate so high?
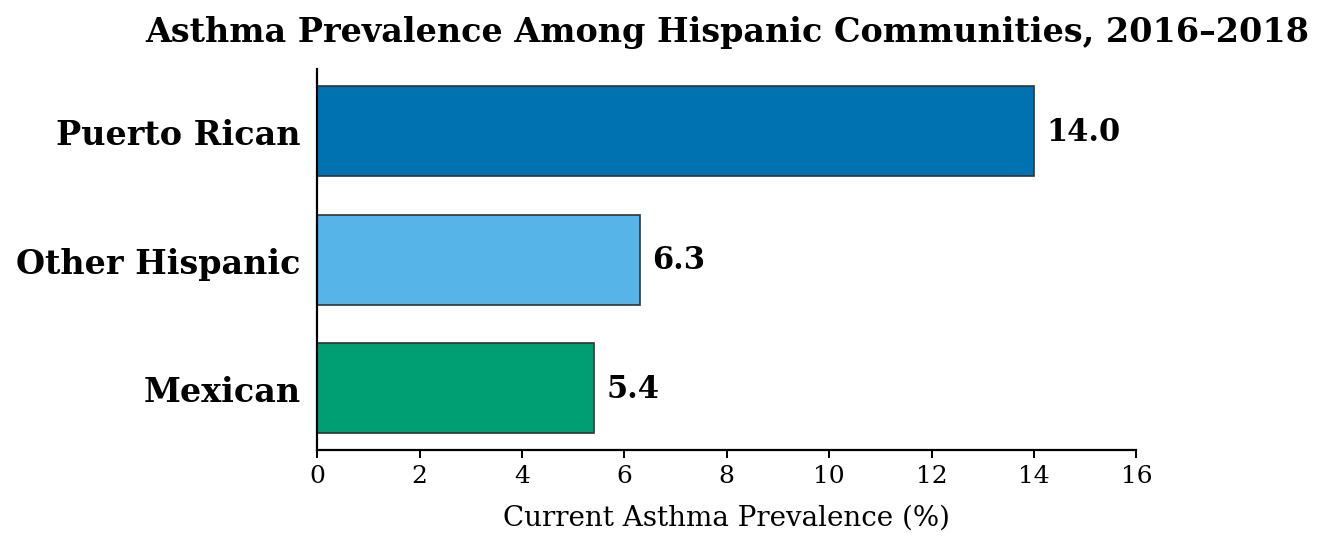
Puerto Ricans have the highest asthma rates of any population group in the country, far exceeding other Hispanic subgroups, a distinction that lumping all Hispanics into one statistic routinely obscures.
Why is their rate so high?
Lower-income individuals and families are more likely to develop and struggle with asthma in the United States.
Lower-income families are more likely to live near pollution, in substandard housing, and farther from specialty care. Cost also prevents many people from obtaining inhalers, medications, and regular treatment. As a result, about half of children and most adults with asthma do not have their disease under control.
Part 2: What Drives These Asthma Disparities?
Asthma is a chronic inflammatory disease of the airways, and nearly everything that drives this inflammation in America is experienced unequally.

What the Evidence Shows:
Abdulrahman Jbaily at American University led a study in TK showing that the higher the concentration of Blacks and Hispanics in a U.S. zip code, the higher the level of air pollution. Conversely, the higher the concentration of Whites, the lower the level of air pollution.
1. Air pollution hits certain communities harder
Poor air quality is the most direct cause of asthma attacks. The communities with the highest burden of asthma are disproportionately located near highways, power plants, and industrial facilities, the result of zoning decisions that concentrated pollution in minority and low-income neighborhoods for generations.
What helps: Stronger air pollution standards, limits on placing polluting industrial facilities near homes and schools, and cleaner energy policies directly reduce asthma-triggering exposures.

What the Evidence Shows:
Elizabeth Matsui of the Johns Hopkins Bloomberg School of Public Health and her colleagues demonstrated that allergens found in mouse urine are widespread in inner-city homes and schools and are strongly associated with asthma symptoms, attacks, emergency visits, and reduced lung function among sensitized children.
Her work helped drive efforts to include pest management in asthma prevention programs.
2. Exposure to indoor asthma triggers is greater in substandard housing conditions.
Indoor asthma triggers are far more common in poorly maintained housing. Mold, cockroach allergens, dust mites, and tobacco smoke disproportionately expose low-income children to dangerous asthma attacks. The same conditions that increase this risk also block solutions: delayed repairs, weak housing code enforcement, and families with little financial or legal power to demand safer homes.
What helps: Home visiting programs that remove mold, pests, excess moisture, and poor ventilation from homes can prevent asthma attacks before they happen. Stronger housing code enforcement and weatherization programs help protect families when landlords fail to make repairs.
What the Evidence Shows:
David Rosenstreich of the Albert Einstein College of Medicine and his colleagues demonstrated in 1997 that inner-city children who were both sensitized to cockroach allergens and heavily exposed to them in their homes experienced more asthma symptoms, missed school days, hospitalizations, and unscheduled medical visits than other children.
This study provided some of the strongest evidence that housing conditions and environmental exposures are a major contributer to asthma disparities in urban communities.
3. Climate change amplifies existing asthma risks
Climate change is worsening asthma risks. Pollen seasons are getting longer, wildfire smoke is spreading farther, and extreme heat is intensifying air pollution. When Canadian wildfire smoke blanketed New York in 2023, asthma ER visits jumped 82 percent — hitting hardest in communities already burdened by the worst air quality.
What helps: Cutting emissions is the long-term answer. Near-term, air quality alerts and HEPA filtration offer partial protection — but neither reaches households that can’t afford the equipment.
4. Emergency room asthma care creates a costly cycle of repeated health emergencies
For many low-income and minority patients, asthma care begins only when breathing becomes a crisis. Barriers to primary care, specialist access, and affordable medications often leave the emergency room as the only option.
While ERs can treat acute attacks, they cannot provide the ongoing management needed to prevent future ones. Without regular follow-up, controller medications, and asthma action plans, patients often return to the same conditions that triggered the attack, creating a costly cycle of repeated emergencies rather than long-term control.
What helps: Medicaid expansion, school-based programs, community health workers, single-inhaler therapy, and telehealth all demonstrably reduce emergency department visits and hospitalizations.
Preventive care remains out of reach for many families
For many low-income and minority patients, asthma care begins only when breathing becomes a crisis. Barriers to primary care, specialist access, and affordable medications often leave the emergency room as the only option.
While ERs can treat acute attacks, they cannot provide the ongoing management needed to prevent future ones. Without regular follow-up, controller medications, and asthma action plans, patients often return to the same conditions that triggered the attack, creating a costly cycle of repeated emergencies rather than long-term control.
What helps: Medicaid expansion, school-based programs, community health workers, single-inhaler therapy, and telehealth all demonstrably reduce emergency department visits and hospitalizations.
5. The cost of asthma control is higher than many families can afford
For many low-income and minority patients, asthma care begins only when breathing becomes a crisis. Barriers to primary care, specialist access, and affordable medications often leave the emergency room as the only option.
While ERs can treat acute attacks, they cannot provide the ongoing management needed to prevent future ones. Without regular follow-up, controller medications, and asthma action plans, patients often return to the same conditions that triggered the attack, creating a costly cycle of repeated emergencies rather than long-term control.
What helps: Medicaid expansion, school-based programs, community health workers, single-inhaler therapy, and telehealth all demonstrably reduce emergency department visits and hospitalizations.
6. Chronic stress increases vulnerability to asthma
For many low-income and minority patients, asthma care begins only when breathing becomes a crisis. Barriers to primary care, specialist access, and affordable medications often leave the emergency room as the only option.
While ERs can treat acute attacks, they cannot provide the ongoing management needed to prevent future ones. Without regular follow-up, controller medications, and asthma action plans, patients often return to the same conditions that triggered the attack, creating a costly cycle of repeated emergencies rather than long-term control.
What helps: Medicaid expansion, school-based programs, community health workers, single-inhaler therapy, and telehealth all demonstrably reduce emergency department visits and hospitalizations.
7. Communities most affected by asthma are least represented in clinical trials of new asthma treatments
When the populations most burdened by asthma are excluded from clinical trials, the treatments, guidelines, and diagnostic tools that result are optimized for patients who are least affected. Clinicians are left without evidence on whether new therapies work in the patients who need them most — deepening a cycle where underserved communities bear the highest burden but receive the least tailored care.
8. Healthcare bias leaves some asthma patients under-diagnosed and under-treated
For many low-income and minority patients, asthma care begins only when breathing becomes a crisis. Barriers to primary care, specialist access, and affordable medications often leave the emergency room as the only option.
While ERs can treat acute attacks, they cannot provide the ongoing management needed to prevent future ones. Without regular follow-up, controller medications, and asthma action plans, patients often return to the same conditions that triggered the attack, creating a costly cycle of repeated emergencies rather than long-term control.
What helps: Medicaid expansion, school-based programs, community health workers, single-inhaler therapy, and telehealth all demonstrably reduce emergency department visits and hospitalizations.
Clinical bias has also shaped asthma care. For decades, spirometry tests that adjusted for race underestimated lung impairment in Black and Hispanic patients, contributing to their underdiagnosis and undertreatment. Although major medical societies now recommend race-neutral standards, many clinics still use older spirometry software built on race-adjusted equations.
What helps: Race-neutral spirometry standards help correct systematic underdiagnosis, while telehealth expands specialist access for patients with limited geographic or financial access to pulmonary care.
Part 3: Solutions That Work
1. Improving air quality for asthma patients
The CDC’s EXHALE program combines home visits to identify and remove asthma triggers, school initiatives to upgrade HVAC systems and move children indoors during unsafe air quality conditions, and coordinates broader clean-air regulations to reduce indoor and outdoor exposure.
The Impact: Reduced asthma-related hospitalizations, emergency department visits, and healthcare costs.
Source: CDC National Asthma Control Program — EXHALE | https://www.cdc.gov/national-asthma-control-program/php/exhale/index.html
2. Lowering exposure to indoor asthma triggers
The NIH-funded Inner-City Asthma Study deployed HEPA air cleaners, allergen-proof bedding, and pest control in lower-income urban homes, with research assistants making up to seven visits to ensure proper implementation.
The Impact: Children experienced nearly 20% fewer symptom days, 20% fewer missed school days, and 14% fewer unscheduled medical visits per year compared to those who did not receive the intervention.
Source: Results of a Home-Based Environmental Intervention among Urban Children with Asthma. New England Journal of Medicine | https://doi.org/10.1056/NEJMoa032097
3. Countering the impact of climate change
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
4. Breaking the cycle of emergency room asthma care
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
5. Lowering the high cost of asthma medications
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
6. Lowering stress among asthma patients
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
7. Broaden the range of asthma patients enrolled in clinical trials
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
8. Addressing healthcare bias towards certain groups
A partnership between the Regional Asthma Management and Prevention (RAMP) program and seven home visiting programs distributed HEPA air purifiers paired with in-home education to low-income residents with poorly controlled asthma in six San Francisco Bay Area counties.
The Impact: Wildfire smoke and particulate matter exposure was reduced for more than 2,000 of the region’s most vulnerable residents.
Source: Regional Asthma Management and Prevention (RAMP) — Public Health Institute https://rampasthma.org/blog/scaling-up-the-distribution-of-air-cleaners-for-low-income-people-with-asthma/
A Final Word
Asthma is one of the most manageable chronic diseases in medicine. The drugs work. The interventions work. The evidence on what drives disparities — and what closes them — is not in dispute. What is in dispute, right now, is whether the country will continue to let ZIP code, race, and income determine who gets to breathe.
If You or Someone Near You Is Having an Asthma Attack
Knowing what to do in the first minutes can make the difference between a manageable episode and a medical emergency. An attack can begin with coughing, chest tightness, wheezing, or lightheadedness.
- Use your reliever inhaler as soon as symptoms start. Sit upright — lying down makes breathing harder — stay as calm as you can, and breathe slowly.
If symptoms don’t improve shortly after using your reliever, seek care. Go to the emergency room if at-home medicines aren’t working.
Seek care right away — don’t wait to see if it improves — if you or your child have been hospitalized for asthma in the past year, have had a life-threatening attack before, or recently needed oral corticosteroids. Call 911 immediately if breathing becomes too labored to speak in full sentences, or if lips or fingernails appear bluish.
Carry a quick-relief inhaler at all times. Working with your provider to create a written asthma action plan in advance is the most reliable way to know exactly what to do when an attack happens.
For full guidance, visit nhlbi.nih.gov/health/asthma/attacks.
