Maternal Mortality
Maternal mortality—the death of a woman during pregnancy, at delivery or within one year after childbirth—is one of the starkest health disparities in the United States. The U.S. has the highest rate among developed nations.
Key Facts
• Some mothers have a much greater risk of dying because of health disparities
• Most maternal deaths occur after delivery, often weeks or months later
• About 80% of maternal deaths are believed to be preventable
• Mortality rates vary dramatically by state



Most Affected
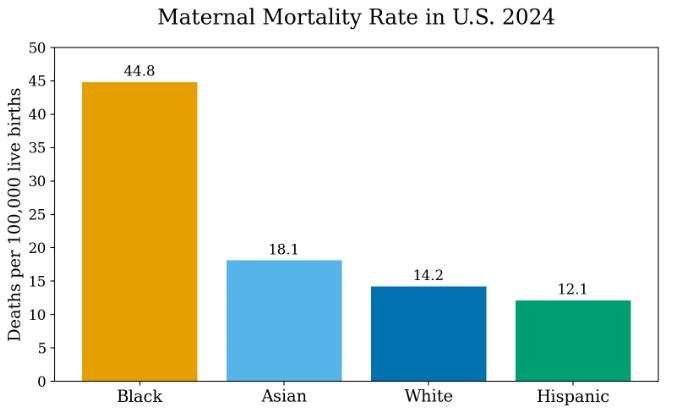
Black mothers die at a rate more than 3 times higher than White mothers.
• Mothers living in rural areas in the US are about twice as likely to die as mothers living in large metropolitan areas.
American Indian and Alaska Native mothers die at a rate more than 8 times higher than White mothers
Why this is a disparity
Maternal mortality is not evenly distributed among women in the United States. The differences persist across income and education levels, indicating that it’s a true health disparity driven by systemic—not biological—factors.
Drivers of Disparities — and What Helps
Unequal Access to High-Quality Health Care
The disparity: Black and Hispanic mothers disproportionately give birth in “safety-net” hospitals, which often face chronic underfunding and resource scarcity. These facilities frequently lack specialized obstetric units and have fewer nurses per patients, directly correlating to increased rates of preventable complications.
Why it matters: Black and Hispanic women face substantially higher risks of severe maternal complications and deaths compared to white women treated at better-resourced, high-volume institutions.
What helps: Expanding postpartum coverage, strengthening hospital capacity, and increasing access to midwives and doulas.
→ See solutions: Coverage expansion, workforce models, and hospital investment
What’s working:
- Extending Medicaid coverage to 12 months postpartum
- Expanding access to midwives, doulas, and community-based providers
- Strengthening hospital capacity in underserved areas
Why it matters:
Continuous coverage and supportive care models improve early detection of complications and ensure follow-up after delivery.
Disparity Disruptor:
States that have extended postpartum Medicaid coverage are seeing improved care continuity, especially for low-income mothers.
2) Differences in Quality of Care
Why it matters: Care varies widely across hospitals and providers, leading to missed warning signs, delayed treatment, and poor coordination.
What helps: Standardized safety protocols and quality improvement collaboratives.
→ See solutions: Patient safety bundles, hospital accountability, and data-driven improvement
3) Structural Racism and Bias
Why it matters: Bias—both implicit and explicit—can affect how symptoms are heard, taken seriously, and treated.
What helps: Bias training, a more diverse workforce, and culturally competent care.
→ See solutions: Workforce diversification, bias reduction strategies, and respectful care models
4) Higher Burden of Chronic Conditions
Why it matters: Conditions such as hypertension and cardiovascular disease increase the risk of pregnancy-related complications.
What helps: Preventive care, early risk screening, and better chronic disease management.
→ See solutions: Preconception care, risk screening programs, and chronic care integration
5) Social and Economic Conditions
Why it matters: Housing, income, food security, and transportation shape access to and continuity of care.
What helps: Stronger social supports and reducing logistical barriers.
→ See solutions: Community-based programs, care navigation, and social needs integration
6) Geographic Inequities
Why it matters: Rural and tribal communities often lack nearby maternity care, increasing delays and risks.
What helps: Telehealth and targeted rural maternity investment.
→ See solutions: Telehealth expansion, rural workforce incentives, and facility funding
7) Postpartum and Mental Health Gaps
Why it matters: Nearly half of maternal deaths occur after delivery, often when coverage lapses and mental health needs go unmet.
What helps: 12-month postpartum coverage and integrated mental health care.
→ See solutions: Postpartum coverage policy, mental health integration, and follow-up care models
8) Cumulative Stress (“Weathering”)
Why it matters: Chronic stress from social and economic disadvantage and racism increases long-term health risks.
What helps: Long-term community and public health investment.
→ See solutions: Community health investment and upstream prevention strategies
Solutions
The United States leads high-income nations in maternal deaths—but most of these deaths don’t have to happen. An estimated 80 percent are preventable, pointing to clear opportunities for change. The strongest solutions target the root causes: gaps in continuous, high-quality care and the social and economic barriers that make it harder for some women to stay healthy. Reducing maternal mortality will require closing these gaps so that whether a woman survives childbirth in the U.S. is not dictated by race, income, or geography.
1) Expanding Access to Continuous, High-Quality Care
What’s working:
- Extending Medicaid coverage to 12 months postpartum
- Expanding access to midwives, doulas, and community-based providers
- Strengthening hospital capacity in underserved areas
Why it matters:
Continuous coverage and supportive care models improve early detection of complications and ensure follow-up after delivery.
Disparity Disruptor:
States that have extended postpartum Medicaid coverage are seeing improved care continuity, especially for low-income mothers.
2) Improving Quality and Safety of Maternal Care
What’s working:
- Standardized safety bundles for obstetric emergencies (e.g., hemorrhage, hypertension)
- Hospital quality improvement collaboratives
- Data tracking and accountability systems
Why it matters:
Consistent use of evidence-based protocols reduces preventable complications and deaths across hospitals.
Disparity Disruptor:
Statewide maternal safety collaboratives have reduced severe complications by standardizing care across diverse hospital systems.
3) Addressing Bias and Improving Patient-Centered Care
What’s working:
- Implicit bias and respectful care training
- Patient advocacy and navigation programs
- Diversifying the maternal health workforce
Why it matters:
Better communication and trust improve early recognition of symptoms and adherence to care.
Disparity Disruptor:
Community-based doula programs have been shown to improve outcomes and patient experience among Black and low-income mothers.
4) Managing Chronic Conditions Before and During Pregnancy
What’s working:
- Preconception care and early risk screening
- Integrated care models that coordinate obstetric and primary care
- Focused management of hypertension and cardiovascular risk
Why it matters:
Reducing underlying health risks before and during pregnancy lowers the likelihood of severe complications.
Disparity Disruptor:
Programs that integrate primary care with maternity services are improving outcomes for high-risk patients.
5) Addressing Social and Economic Barriers
What’s working:
- Transportation and care navigation support
- Group prenatal care models
- Policies addressing food, housing, and income stability
Why it matters:
Reducing logistical and financial barriers helps mothers access consistent, timely care.
Disparity Disruptor:
Group prenatal care models (e.g., CenteringPregnancy-style programs) have improved engagement and outcomes in underserved communities.
6) Expanding Care in Underserved and Rural Areas
What’s working:
- Telehealth for prenatal and postpartum visits
- Investment in rural maternity units and workforce
- Targeted support for tribal and frontier communities
Why it matters:
Access to care—especially in emergencies—depends heavily on geography.
Disparity Disruptor:
Telehealth expansion has improved access to specialists for rural and remote populations.
7) Strengthening Postpartum and Mental Health Care
What’s working:
- Extended postpartum coverage and follow-up care
- Screening for depression, anxiety, and substance use
- Integration of behavioral health into maternal care
Why it matters:
A significant share of maternal deaths occur after delivery, often linked to untreated mental health or medical conditions.
Disparity Disruptor:
Programs that embed mental health care into postpartum visits are increasing detection and treatment of high-risk conditions.
8) Investing in Long-Term Community Health
What’s working:
- Community health worker programs
- Long-term investments in neighborhood health and resources
- Cross-sector partnerships addressing structural inequities
Why it matters:
Maternal health outcomes are shaped long before pregnancy begins.
Disparity Disruptor:
Community-led health initiatives are helping reduce risk by addressing chronic stress and long-term health conditions.
Where Progress Is Happening
- California — Maternal safety collaboratives significantly reduced mortality rates
- North Carolina — Community health worker and care coordination models improving outcomes
- Multiple states nationwide — Adoption of 12-month postpartum Medicaid coverage
- Tribal health systems — Expanding culturally tailored maternal care programs
Final Bottom Line
Maternal mortality disparities are not inevitable—they are the predictable result of systemic gaps in care, access, and equity.
Because most maternal deaths are preventable, this disparity represents one of the clearest examples of avoidable harm in the U.S. healthcare system.
The challenge is not identifying solutions—it is scaling what works and ensuring it reaches those most at risk.
How These Solutions Fit Together
No single intervention is sufficient. The most effective approaches:
- Combine clinical improvements + social supports
- Focus on continuity of care before, during, and after pregnancy
- Target both healthcare systems and underlying inequities
Bottom Line
The evidence is clear:
Maternal mortality disparities are not inevitable—they are responsive to policy, healthcare system improvements, and community-based interventions.
The challenge is not identifying solutions.
It is scaling what works and ensuring it reaches the populations most at risk.